Recovery of upper limb muscle function in chronic fatigue syndrome with and without fibromyalgia.
Eur J Clin Invest. 2013 Nov 11. doi: 10.1111/eci.12201. [Epub ahead of print]
Ickmans K1, Meeus M, De Kooning M, Lambrecht L, Nijs J.
Author information
Abstract
BACKGROUND:
Chronic fatigue syndrome (CFS) patients frequently complain of muscle fatigue and abnormally slow recovery, especially of the upper limb muscles during and after activities of daily living.
Furthermore, disease heterogeneity has not yet been studied in relation to recovery of muscle function in CFS.
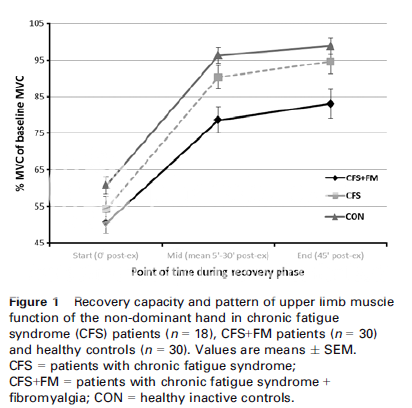
Here, we examine recovery of upper limb muscle function from a fatiguing exercise in CFS patients with (CFS+FM) and without (CFS-only) comorbid fibromyalgia and compare their results with a matched inactive control group.
DESIGN:
In this case-control study, 18 CFS-only patients, 30 CFS+FM patients and 30 healthy inactive controls performed a fatiguing upper limb exercise test with subsequent recovery measures.
RESULTS:
There was no significant difference among the three groups for maximal handgrip strength of the non-dominant hand.
A significant worse recovery of upper limb muscle function was found in the CFS+FM, but not in de CFS-only group compared with the controls (P < 0·05).
CONCLUSIONS:
This study reveals, for the first time, delayed recovery of upper limb muscle function in CFS+FM, but not in CFS-only patients.
The results underline that CFS is a heterogeneous disorder suggesting that reducing the heterogeneity of the disorder in future research is important to make progress towards a better understanding and uncovering of mechanisms regarding the nature of divers impairments in these patients.
KEYWORDS:
Chronic fatigue syndrome, handgrip strength, maximal voluntary contraction, muscle fatigue, muscle recovery
PMID: 24313704 [PubMed - as supplied by publisher]