
I am homozygous for MTR A2756G (rs1805087) and I realized I failed to look at the details about this mutation carefully. If I did my calculations correctly from dbSNP, it appears that only 1.7% of Europeans are homozygous for this (I am 100% European). Pretty rare!
http://www.ncbi.nlm.nih.gov/SNP/snp_ref.cgi?searchType=adhoc_search&type=rs&rs=rs1805087
So my questions are, what more can I do about this them supplementing massive amounts of methyl-B12. I have added folate, P5P, etc, but it’s been pretty clear the last couple years that the biggest need is methyl-B12. In fact, I feel that I actually could die without it even thoiugh my lab results are >1999 for B12. It makes a huge difference. While not functional in terms of having a job, exercise, etc it helps me immensely compared to how I would be without it (incapacitated).
I have seen megoblastic anemia when I was feeling really sick or stopped B12 for a significant period of time.
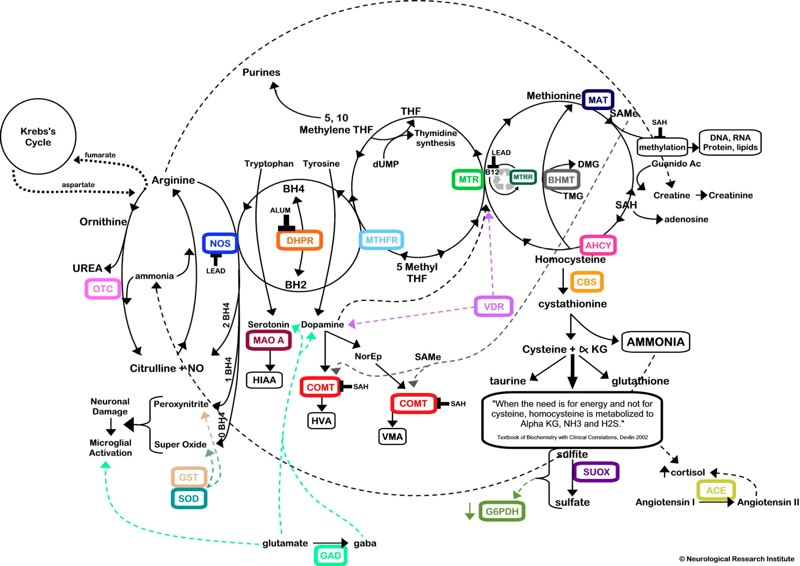
I also wanted to know how heavy metals would be implicated. On the diagram below, it looks like MTRR recycles B12. I also see with word “lead” there, and was wondering if the diagram is talking about lead as in the heavy metal. I am heterozygous for MTRR A66G, but I don’t know how much weight that has. But my question is, is this implying that I could have bioaccumulated lead my entire life if there wasn’t much methyl-B12 to be recirculated by MTRR.
I have had depression a few times in my life. However, I was pretty healthy and very active until I suddenly got very sick one day in December 2008. It’s worth noting that the water company where I lived was seized by the government where I lived for high levels of inorganic arsenic and the whole infrastructure (including every single pipe that fed thousands of homes) had to be replaced. I drank the tap water (it was well water). I suffer from chronic infections, anxiety but not depression, chest pain, head pain, other pains that come and go, impaired cognitive processing (hard to drive a car), overstimulation, and so on.
http://www.ncbi.nlm.nih.gov/SNP/snp_ref.cgi?searchType=adhoc_search&type=rs&rs=rs1805087
So my questions are, what more can I do about this them supplementing massive amounts of methyl-B12. I have added folate, P5P, etc, but it’s been pretty clear the last couple years that the biggest need is methyl-B12. In fact, I feel that I actually could die without it even thoiugh my lab results are >1999 for B12. It makes a huge difference. While not functional in terms of having a job, exercise, etc it helps me immensely compared to how I would be without it (incapacitated).
http://en.wikipedia.org/wiki/5-Methyltetrahydrofolate-homocysteine_methyltransferaseMutations in the MTR gene have been identified as the underlying cause of methylcobalamin deficiency complementation group G, or methylcobalamin deficiency cblG-type.[1] The consequence of reduced methionine synthase activity is megaloblastic anemia.
I have seen megoblastic anemia when I was feeling really sick or stopped B12 for a significant period of time.
I also wanted to know how heavy metals would be implicated. On the diagram below, it looks like MTRR recycles B12. I also see with word “lead” there, and was wondering if the diagram is talking about lead as in the heavy metal. I am heterozygous for MTRR A66G, but I don’t know how much weight that has. But my question is, is this implying that I could have bioaccumulated lead my entire life if there wasn’t much methyl-B12 to be recirculated by MTRR.
I have had depression a few times in my life. However, I was pretty healthy and very active until I suddenly got very sick one day in December 2008. It’s worth noting that the water company where I lived was seized by the government where I lived for high levels of inorganic arsenic and the whole infrastructure (including every single pipe that fed thousands of homes) had to be replaced. I drank the tap water (it was well water). I suffer from chronic infections, anxiety but not depression, chest pain, head pain, other pains that come and go, impaired cognitive processing (hard to drive a car), overstimulation, and so on.