Dx Revision Watch
Suzy Chapman Owner of Dx Revision Watch
- Messages
- 3,061
- Location
- UK
I've been asked in addition to "MUS", what other diseases and conditions are the current focus for provision of integrated psychological therapies.
"As set out in Implementing the Five Year Forward View for Mental Health the expansion of Improving Access to Psychological Therapies (IAPT) services will focus on people with long term conditions or medically unexplained symptoms.
"New psychological therapy provision will see physical and mental health care provision co-located.
"Therapy will be integrated into existing medical pathways and services – either primary care, or secondary care services (eg diabetes, cardiac, respiratory)."
https://www.england.nhs.uk/mentalhealth/adults/iapt/mus/sites/
The NHS "Integrated IAPT early implementers" page briefly describes 22 projects across the country which between them are building on existing services or developing new integrated provision for the following:
Long Term Conditions (LTCs), specifically:
chronic obstructive pulmonary disease (COPD)
respiratory disease
asthma
coronary heart disease
cardiac rehabilitation
cardiovascular disease
stroke
diabetes
pre diabetes
cancer
obesity
eczema and psoriasis
dementia care
perinatal
chronic pain management
musculoskeletal conditions
irritable bowel syndrome
chronic fatigue syndrome and ME
medically unexplained symptoms (MUS)
(which may include FM, IBS, CFS, ME)
A Call to bid for Transformation Funding to support the implementation of the Five Year Forward View closed on 18 January 2017. Notification of investment decisions is scheduled for March 2017.
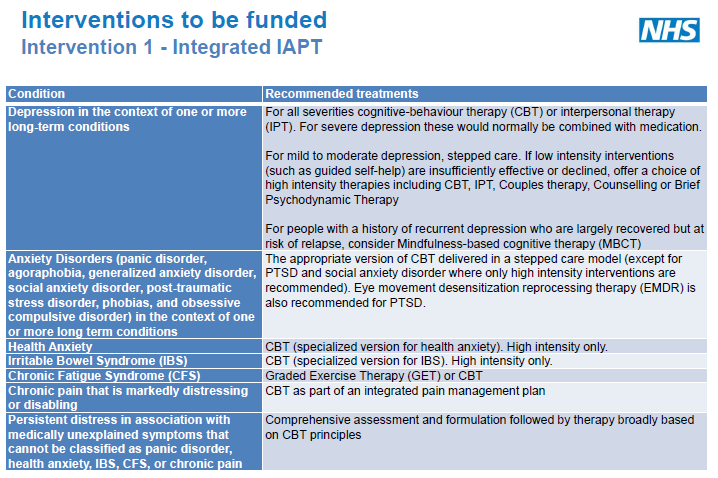
The interventions for which transformation funding is available for Improving access to psychological therapies (Integrated IAPT) are:
Depression in the context of one or more long-term conditions
Anxiety Disorders (panic disorder, agoraphobia, generalized anxiety disorder,
social anxiety disorder, post-traumatic stress disorder, phobias, and obsessive
compulsive disorder) in the context of one or more long-term conditions
Health Anxiety
Irritable Bowel Syndrome (IBS)
Chronic Fatigue Syndrome (CFS)
Chronic pain that is markedly distressing or disabling
Persistent distress in association with medically unexplained symptoms that
cannot be classified as panic disorder, health anxiety, IBS, CFS, or chronic pain
"As set out in Implementing the Five Year Forward View for Mental Health the expansion of Improving Access to Psychological Therapies (IAPT) services will focus on people with long term conditions or medically unexplained symptoms.
"New psychological therapy provision will see physical and mental health care provision co-located.
"Therapy will be integrated into existing medical pathways and services – either primary care, or secondary care services (eg diabetes, cardiac, respiratory)."
https://www.england.nhs.uk/mentalhealth/adults/iapt/mus/sites/
The NHS "Integrated IAPT early implementers" page briefly describes 22 projects across the country which between them are building on existing services or developing new integrated provision for the following:
Long Term Conditions (LTCs), specifically:
chronic obstructive pulmonary disease (COPD)
respiratory disease
asthma
coronary heart disease
cardiac rehabilitation
cardiovascular disease
stroke
diabetes
pre diabetes
cancer
obesity
eczema and psoriasis
dementia care
perinatal
chronic pain management
musculoskeletal conditions
irritable bowel syndrome
chronic fatigue syndrome and ME
medically unexplained symptoms (MUS)
(which may include FM, IBS, CFS, ME)
A Call to bid for Transformation Funding to support the implementation of the Five Year Forward View closed on 18 January 2017. Notification of investment decisions is scheduled for March 2017.
The interventions for which transformation funding is available for Improving access to psychological therapies (Integrated IAPT) are:
Depression in the context of one or more long-term conditions
Anxiety Disorders (panic disorder, agoraphobia, generalized anxiety disorder,
social anxiety disorder, post-traumatic stress disorder, phobias, and obsessive
compulsive disorder) in the context of one or more long-term conditions
Health Anxiety
Irritable Bowel Syndrome (IBS)
Chronic Fatigue Syndrome (CFS)
Chronic pain that is markedly distressing or disabling
Persistent distress in association with medically unexplained symptoms that
cannot be classified as panic disorder, health anxiety, IBS, CFS, or chronic pain
Last edited:
 and high moral standards
and high moral standards