This comment has undergone substantial editing since initial posting.
The NCHS/CMS ICD-10-CM update and revision mechanism is a public process.
Requests for additions or modifications to ICD-10-CM/PCS are tabled in meeting Agendas (or Topic Packets as they are known). The public can register to attend meetings in person, or participate via phone link. Meetings are web-cast live and videos of both days’ proceedings are posted, followed by the posting of a meeting summary and public comment period (of between 3 to 8 weeks) through which comments and objections to requests for modifications presented at the most recent meeting can be submitted.
But the WHO-FIC’s
ICD-10 Update and Revision process is
not a public process.
It would not be easy to monitor the progress of any potential request submitted to the
WHO-FIC Update and Revision Committee via the
North American WHO-FIC Collaborating Center or
Collaborating Centers for Classifications, Terminologies and Standards (or any other countries' WHO-FIC Network Collaborating Centres) unless the agencies steering any request and its progress placed information in the public domain.
If a request for inclusion in WHO's ICD-10 were to be made by the agencies with a stake in the IOM's recommendations, via the U.S. Collaborating Centers, I think it unlikely that any request would be submitted until
after SEID had been adopted, approved for insertion into ICD-10-CM and preparations for its dissemination and implementation within the U.S. were well advanced.
By then, we could be looking at 2016+ if not longer. (I haven't noted any projected timeline within the Report's recommendations.)
I would envisage the URC rejecting any proposal for adding SEID to WHO's ICD-10 in preference to consideration for inclusion within the ICD-11 Beta draft (either coded for or included under the list of Synonym terms) or for consideration for inclusion within the next annual update of ICD-11, if the ICD-11 version for 2017 had already been ratified by WHA and released.
The update cycle for ICD-10 has been:
Tabular list: Every three years for major changes, annually for minor changes.
Index: Annually for changes that do not impact on the structure of the tabular list.
What constitutes a Major or Minor change is set out on Page 3 of this
document.
However, it may be that the U.S. agencies with a stake in SEID do not see their remit extending to the colonization of classification systems beyond the U.S. Though they may conceivably apply for inclusion of the SEID term within the U.S. extension of SNOMED CT and the U.S. SNOMED CT code to ICD-10-CM code cross-walk.
CDC's Donna Pickett* co-chairs the NCHS/CMS
Coordination and Maintenance Committee meetings. In 2010-11, when U.S. advocates submitted proposals via the C & M meetings for shifting CFS out of the Chapter 18 R codes and back under Chapter 6 under G93.3, where it had originally been proposed to be located, Ms Pickett put up considerable barriers to change. Committee elected to stick with the status quo.
Given Ms Pickett's opposition to these proposals for changing the location of CFS, several years ago, it will be interesting to see how she deals with any future submission on behalf of IOM contract stakeholders for the insertion of SEID into ICD-10-CM.
*WHO Collaborating Centre for WHO-FIC in North America; Voting Member, WHO-FIC Update and Revision Committee (URC).
ICD-11
As far as ICD-11 is concerned, stakeholders need to register with the Beta draft for enhanced interaction with the drafting platform, for access to additional resources and in order to submit proposals for addition of new entities or suggest content changes to existing entities, via the Proposal Mechanism. New proposals to the evolving Beta draft are generated internally by the Topic Advisory Groups and externally by medical professional bodies, clinicians, researchers, allied medical professionals and other interested stakeholders.
Proposals are then subject to review by the chairs and managing editors of the appropriate Topic Advisory Groups (TAGs), sometimes to external review, and by the RSG. Proposals that are approved, provisionally, are then entered into the Beta draft and marked as “Implemented” in the Proposal Mechanism.
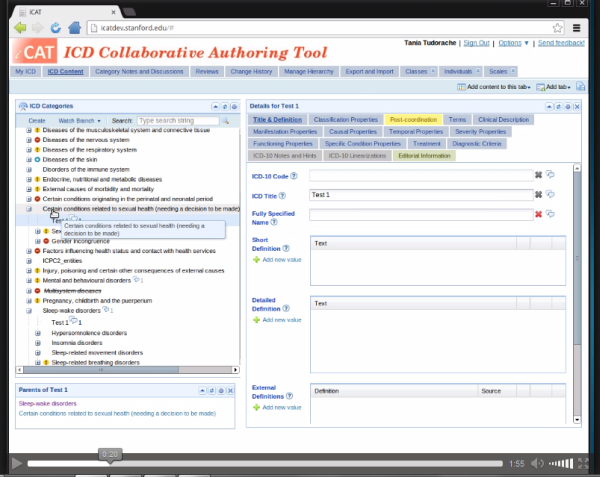
One can follow the status of proposals via the Proposal Mechanism. But one cannot view the TAGs’ rationales or Discussion Notes (ie the decision making process) that results in the Approval or Rejection of a specific proposal. These Discussion Notes are only available to those with editing access to the more complex iCAT authoring platform that the ICD working groups are using to develop the draft on, which looks like this:
If you look closely, you'll see that at the point at which this screencast was posted by a member of the iCAT editors Google Group the dropdown for "Multisystem diseases" had a strike-through.
For comparison between the public Beta draft and the complexity of the iCAT, view this 2 minute iCAT screencast animation (with audio), intended as a demo for ICD Revision editors. The animation is an .ogv file format which should run in recent releases of Firefox but may not load in other browsers.
Proposals for new entities to the public version of the Beta draft need to be supported with rationales and references. In theory, any registered stakeholder could propose the addition of the SEID term and construct to ICD-11, supported by rationales and references. A proposal would not have to come from HHS, IOM, per se, or from any other stakeholder agency.
(Or, when ICD-11 does restore the three ICD-10 legacy terms to the draft, for SEID to be proposed as a specified Inclusion term to whichever ICD-10 legacy term may be designated as the ICD-11 "Title term," or listed under Synonyms to a Title term, if not proposed to be inserted under a discrete new code or if not proposed to replace or subsume one or more of the legacy ICD-10 terms.)
Once ICD-11 has been disseminated, it will be subject to an annual update and revision process, though it is expected that proposals will be considered as soon as they arrive and if approved, added to an annual updated release (as
ICD-11 2018,
ICD-11 2019 and so on).
Suzy Chapman for Dx Revision Watch