Mary Schweitzer: Medical Classification WHO ICD codes (Co-Cure)
May be reposted
Co-Cure URL:
https://listserv.nodak.edu/cgi-bin/wa.exe?A2=ind1110b&L=co-cure&T=0&P=6274
From: "Mary Schweitzer"
To: Co-Cure
Friday, October 14, 2011 2:11 AM
Subject: [CO-CURE] ACT: Medical Classification WHO ICD codes
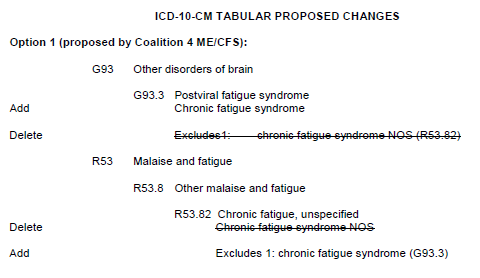
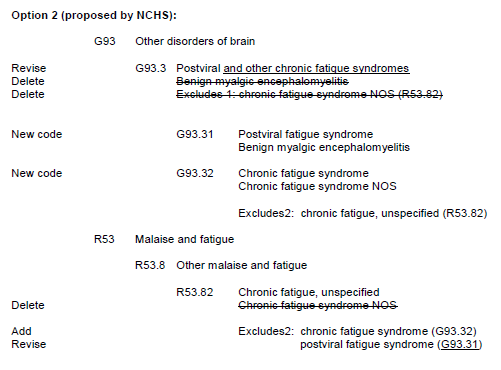
There has of late been speculation that it would be bad for U.S. patients if CFS and M.E. were placed in the same category in the neurology chapter of ICD-10-CM, the "clinical manual" of ICD-10 that will be adopted for use in the United States.
But the fact of the matter is that in ICD-10, CFS already IS coded to G93.3, "PVFS and M.E." in the index, which is as authoritative as the tabular version. [PVFS stands for Post-Viral Fatigue Syndrome, and is not diagnosed very frequently any more - not at all in the U.S.]. It already IS coded in neurology.
110 nations use ICD-10 as-is, including the UK. Australia has a clinical version that does not alter the codes for M.E. or CFS. But Canada and Germany have clinical versions that place CFS in the tabular version of ICD-10, in G93.3 with M.E. In fact, it was the Canadian clinical version, ICD-10-CA, which led to the highly regarded Canadian Consensus Criteria for ME/CFS in 2003.
NOBODY EXCEPT THE UNITED STATES CODES CFS IN THE "R" CHAPTER. If we coded CFS at R53.82, which was the plan of NCHS, we would have been the ONLY nation in the world to do so.
Furthermore, M.E. is not a known diagnosis in the U.S. (WE know about it, but very few doctors do.) There is no definition for it approved by CDC. We can now point to the new definition that was published in the Journal of Internal Medicine, but that is more likely to enable researchers in the US and Canada to use M.E. if they want to, than to trickle down to U.S. clinicians. Part of the problem is that when M.E. replaced atypical polio as a disease name in British commonwealth nations and Europe, in the U.S. the new name was epidemic neuromyesthenia, which has not (to my knowledge) been diagnosed in decades.
So if CFS gets coded as R53.82 in the U.S.'s ICD-10-CM, yes, M.E. will be less likely to confuse with CFS - but that would only be in the U.S., and in the U.S. we only get diagnosed with that revolting name CFS anyway. At least we could get them scratching their heads and asking, "What is M.E.?" if both diseases were placed together where those of you outside the U.S. already have it.
Given that U.S. doctors do not have a high opinion of CFS, keeping it under "R" in "vague signs and symptoms" would only reinforce their prejudice against it as a "garbage diagnosis" - something you diagnose when you run out of ideas.
Finally, there was an inadvertent error in an earlier Co-Cure message about getting CFS out of the "R" category. The "R" category is not for psychiatric diagnoses.
British psychiatrists use "fatigue syndrome," which is coded at F48.0 under neuroses at "neurasthenia.". Then when they write about it, they mix and match terms so it looks as if CFS is the same thing, and therefore it goes in F48.0. That is a serious problem in the UK. [I have to admit to being alarmed recently when a U.S. virologist connected CFS not to the history of post-polio syndrome, which is pretty well established, but to the arcane nineteenth century diagnosis of neurasthenia. Please don't do that!]
We are not (I hope) in current danger of being coded under neuroses at F48.0, neurasthenia, in the U.S. But the "R" diagnosis is sufficiently vague that it wouldn't be difficult to use it to claim CFS patients really have CSSD (Complex Somatic Symptom Disorder), the category British psychiatrist and CBT advocate Michael Sharpe is trying to shoehorn into DSM-5, the new version of the American Psychiatric Association's huge diagnostic tome. So it does leave us vulnerable.
To those outside the US I would say, look to ICD-11. That's what will affect you the most. To those in the US (where we are finally getting around to adopting ICD-10-CM two decades after ICD-10 was written), what WE need is simply to get in step with the rest of the world now.
Mary M. Schweitzer
---------------------------------------------
Send posts to
CO-CURE@listserv.nodak.edu
Unsubscribe at
http://www.co-cure.org/unsub.htm
Too much mail? Try a digest version. See
http://www.co-cure.org/digest.htm
---------------------------------------------
Co-Cure's purpose is to provide information from across the spectrum of
opinion concerning medical, research and political aspects of ME/CFS and/or
FMS. We take no position on the validity of any specific scientific or
political opinion expressed in Co-Cure posts, and we urge readers to
research the various opinions available before assuming any one
interpretation is definitive. The Co-Cure website <www.co-cure.org> has a
link to our complete archive of posts as well as articles of central
importance to the issues of our community.
---------------------------------------------