I have another theory. What if there is a very large increase in intracellular choline and
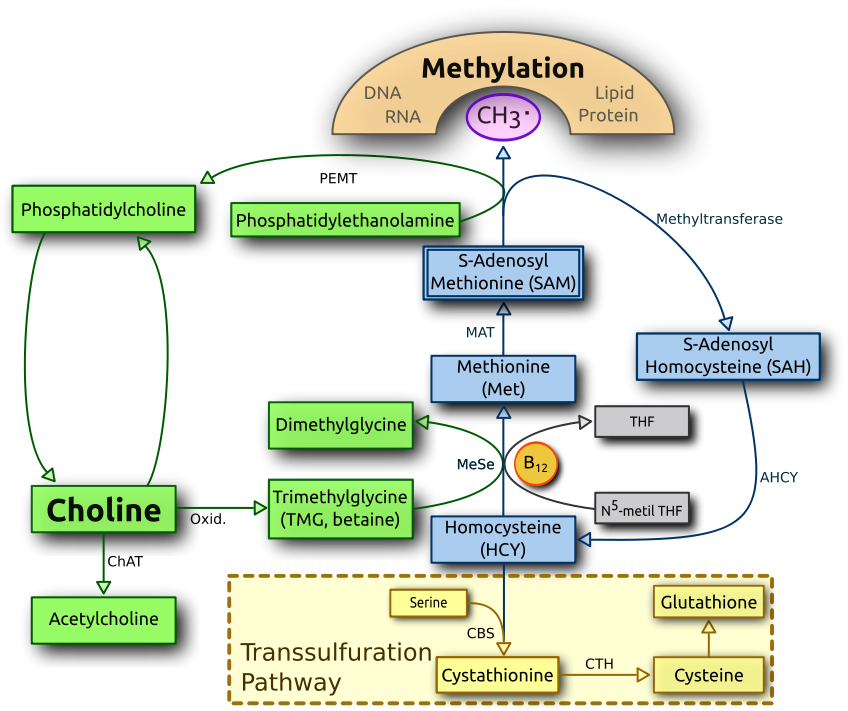
betaine-homocysteine methyltransferase which then crowds out b12 and creates a functional folate deficiency?
Perhaps this can explain why people get fatigue from racetams, which increase choline uptake into cells? And also depression from excess choline supplementation?
Personally I experienced terrible side effects from fasoracetam, which is a drug that heavily increases
high affinity choline uptake. This takes up extracellular choline and puts it into cells.
Another side effect from excess choline would be a lowered amount of acetyl-CoA through
ChAT. Acetyl-CoA also is essential to the Kreb cycle. Acetyl groups are taken from acetyl-coa for every acetylcholine neurotransmitter.
I had severe depression and fatigue before I got CFS. I experimented with stuff like bacopa, DMAE, Alcar, aniracetam, noopept, all of which have effects on choline.
I also had pericarditus and bouts of severe sickness during this time, and those are more likely the problem, but still I have a nagging doubt in my mind that nootropics were a factor. What if oxidative stress from my illness depleted b12, and then nootropics increased intracellular choline, causing cells to swap to TMG instead of folate for methyl groups?
I wonder if reduced choline intake into cells would increase the efficacy of b12? If only there was an easy way to do this, I can't find anything.
EDIT:
https://en.wikipedia.org/wiki/Choline_transporter
And there is also a
choline transporter to mitochondria, which is where choline gets oxidized into TMG.
Turns out
Hemicholinium-3 inhibits choline uptake. Not sure if safe in humans.
I also am wondering if the gut microbiome can supply choline, I remember seeing that some gut bacteria create acetylcholine.