
Jesse2233
Senior Member
- Messages
- 1,942
- Location
- Southern California
Hey everyone,
A bit overwhelmed with my CardioION results from Genova. Any help would be greatly appreciated!
Caveats: Is Genova reliable? Supplementing at the time. Snapshot in time.
Other relevant info: ill 3 months at time of blood draw, high Coxsackie B4 titers, low ANA
Krebs cycle problems
Pre-illness these levels were normal
High aminos
Other abnormalities
Full results:






A bit overwhelmed with my CardioION results from Genova. Any help would be greatly appreciated!
Caveats: Is Genova reliable? Supplementing at the time. Snapshot in time.
Other relevant info: ill 3 months at time of blood draw, high Coxsackie B4 titers, low ANA
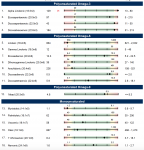
Krebs cycle problems
- Pyruvate is off the charts = 15.9 (reference range <= 6.4)
- L-lactic is low = 0.1 (reference range 0.6 - 16.4)
- Also low cis-aconitate and isocitrate
Pre-illness these levels were normal
- High insulin, triglycerides
High aminos
- High lysine, methione, tryptophan, isoleucine, leucine, valine, phenylaline, histidine, threonine, arginine, serine
Other abnormalities
- Lowish zinc and copper
- High alpha linolenic
- High capric, lauric, and behenic
Full results:
Attachments

Last edited:
