deleder2k
Senior Member
- Messages
- 1,129
Looking for answers to ME riddle
Research 5. MARCH 2015
What exactly is ME? And how can the disease be treated? The Kavli Trust supports cancer researchers at Haukeland University Hospital, Norway, in their pursuit of the answer.
Teresa Grøtan (text and photos)
Chief Physician Øystein Fluge and head of the cancer ward and Professor Olav Mella has previously conducted several studies of cancer drug rituximab on ME patients. Their latest completed study has been sent in for approval to a scientific journal.

PHOTO: Department and Professor Olav Mella, national project coordinator and nurse Kari Sørland and physician and cancer researcher Øystein Fluge trying to figure out what they, and how the disease can be treated. Their hypothesis is that it is a variant of an autoimmune disease that affects the body's ability to control blood flow.
Holes in medical science- ME is a hole in medicine that we will be to close, and we think we’re getting somewhere, says Øystein Fluge.
Fluge has patients experiencing lactic acid after holding a book, patients who feel they have ran a marathon after going to the mail box, and patients who are describing brain fog after mental activity. For many patients sleep doesn’t help at all.
- It surprised us when we became aware of this disease, how similar patients are actually in clinical appearance. It causes us to believe that there is a common disease mechanism behind, and that it is possible to track down. That is what drives us, says Olav Mella.
Genetic predisposition
Mella, Fluge and national project coordinator and nurse Kari Sørland think ME is a variant of autoimmune disease, i.e. a disease where the body attacks itself.
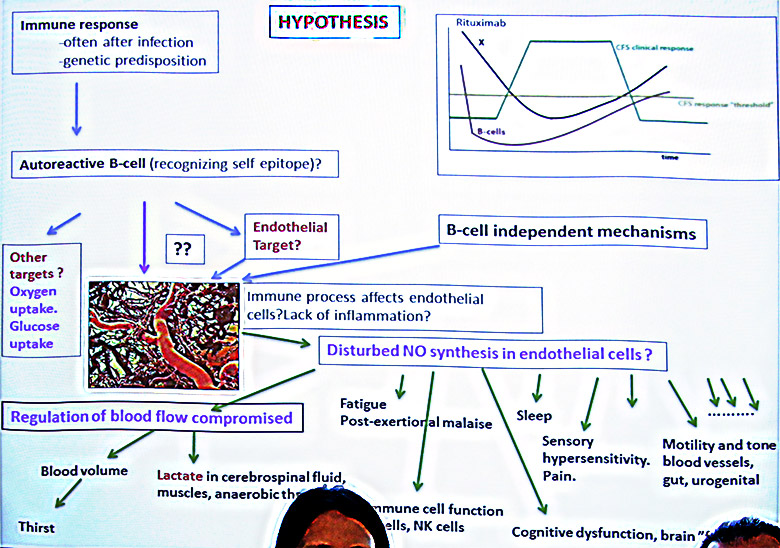
- We believe that it is an auto-reactive response, often after an infection, which in one way or another disrupts the body's ability to fine-tune blood flow, says Fluge.
An indication of this is that the blood vessels in ME patients does not expand as much as in healthy after completing a test where blood vessels are squeezed together.
The researchers also believe that there is a genetic predisposition to ME.
- We see that there is an accumulation in some families. Among those who participated in the first study, 45 percent of autoimmune diseases in their close family. This is higher than in the general population, says Fluge.
Two new studies
The team at Haukeland has started to test the drug rituximab in a large, randomized test over three years in five treatment centers in the country. 152 ME patients in the study, which is called double blind, meaning that neither the patient nor the staff knows about whether the patient receive saline or medicine.
The three are excited about the result, but equally excited about the results of another study that they also will initiate this year with another medicine, used in cancer therapy called cyclophosphamide.
Two breast cancer patients who also had prolonged ME, experienced a major improvement after treatment with cyclophosphamide.
Following these observations doctors gave cyclophosphamide to three ME patients without cancer. Two of them experienced a major improvement. One of these was mainly bedridden. Before treatment, one patient walked on average 326 steps a day. After six infusions of cyclophosphamide she walked 13,000 steps a day.
- We do not know whether the three patients are representative for a larger group of ME patients, but we believe that the observations can justify a clinical trial, says Fluge
The study using cyclophosphamide with six infusions, and with follow-up of 12 months, has just been approved by the Ethics Committee and the Medicines Agency. The three stressed that they have already found the patients who will participate.
- We have received letters from various parts of the world to participate in this survey. I keep getting SMS’ and emails from desperate people who ask for help, telling Fluge.
Want to reach the very sickest
40 patients, all moderately or severely ill ME, will try out the medicine. At least 25 patients will be "new", without prior rituximab treatment, while up to 15 may have gotten rituximab earlier, either without response or relapse.
- If we have a minimum 40 percent response rate among the 25 patients who have not received treatment earlier, then we will start the second part of the study, where we will try the treatment of patients who are so ill that they for years have remained at home or in nursing homes complete darkness and silence, Fluge says.
This part of the study is conceived as a collaboration between Haukeland University and local health care providers.
The Kavli Trust supports the cyclophosphamide study with a 50 percent nursing position for 12 months. The trust also finances the laboratory work related to both rituximab- and cyclophosphamide studies. The hospital does blood work of all patients included in both studies. The samples are analyzed and submitted to a bio bank.
Wants to understand disease mechanism The researchers also conducted three autopsies of people who suffered from ME.
- We are trying to understand disease mechanism. Intellectually, this work is just as interesting as watching response to disease treatment. It is this that can remove the whole management of the disease and the patient group, says Olav Mella.
Scientists estimate that 0.1-0.2 percent of the population are affected ME.
They differ between ME, defined by so-called Canadian criteria, and fatigue and burnout that can befall ten times more than those diagnosed by strict criteras. They think a lot of disagreements that have emerged is due to what one define ME to be.
- It is fascinating that some claim they are sure what ME is. We do not know what ME is. We have some hypotheses, but we do not know. There is no proof of what ME is as of today. On that basis, it is interesting that some ignore what patients has to say about their illness, says project coordinator Kari Sørland.
- We can understand that one can disagree our hypothesis for ME. However, it is incomprehensible that some rejects the idea of research and clinical trials, if these are thoughtful and performed by international guidelines, says Fluge.
From faker's disease to plaque in the brain
ME is not the first disease in history where the sick have not been believed. Multiple sclerosis (MS) was called faker's disease until the MRI apparatus was invented and found plaques in the brain. Ulcers believed came because of stress, until it was discovered a bacterium in the stomach.
Because of the high costs it is rare that such large trials that the new rituximab study is researcher driven and not initiated and run by pharmaceutical companies. The research team has received support from the Ministry of Health, the Research Council, ME Association, fundraising MEandYou besides the Kavli Trust.
Original article in Norwegian: http://kavlifondet.no/2015/03/leter-etter-svar-pa-me-gaten/
(Translated by myself with some help from Google Translate)
Research 5. MARCH 2015
What exactly is ME? And how can the disease be treated? The Kavli Trust supports cancer researchers at Haukeland University Hospital, Norway, in their pursuit of the answer.
Teresa Grøtan (text and photos)
Chief Physician Øystein Fluge and head of the cancer ward and Professor Olav Mella has previously conducted several studies of cancer drug rituximab on ME patients. Their latest completed study has been sent in for approval to a scientific journal.
PHOTO: Department and Professor Olav Mella, national project coordinator and nurse Kari Sørland and physician and cancer researcher Øystein Fluge trying to figure out what they, and how the disease can be treated. Their hypothesis is that it is a variant of an autoimmune disease that affects the body's ability to control blood flow.
Holes in medical science- ME is a hole in medicine that we will be to close, and we think we’re getting somewhere, says Øystein Fluge.
Fluge has patients experiencing lactic acid after holding a book, patients who feel they have ran a marathon after going to the mail box, and patients who are describing brain fog after mental activity. For many patients sleep doesn’t help at all.
- It surprised us when we became aware of this disease, how similar patients are actually in clinical appearance. It causes us to believe that there is a common disease mechanism behind, and that it is possible to track down. That is what drives us, says Olav Mella.
Genetic predisposition
Mella, Fluge and national project coordinator and nurse Kari Sørland think ME is a variant of autoimmune disease, i.e. a disease where the body attacks itself.
- We believe that it is an auto-reactive response, often after an infection, which in one way or another disrupts the body's ability to fine-tune blood flow, says Fluge.
An indication of this is that the blood vessels in ME patients does not expand as much as in healthy after completing a test where blood vessels are squeezed together.
The researchers also believe that there is a genetic predisposition to ME.
- We see that there is an accumulation in some families. Among those who participated in the first study, 45 percent of autoimmune diseases in their close family. This is higher than in the general population, says Fluge.
Two new studies
The team at Haukeland has started to test the drug rituximab in a large, randomized test over three years in five treatment centers in the country. 152 ME patients in the study, which is called double blind, meaning that neither the patient nor the staff knows about whether the patient receive saline or medicine.
The three are excited about the result, but equally excited about the results of another study that they also will initiate this year with another medicine, used in cancer therapy called cyclophosphamide.
Two breast cancer patients who also had prolonged ME, experienced a major improvement after treatment with cyclophosphamide.
Following these observations doctors gave cyclophosphamide to three ME patients without cancer. Two of them experienced a major improvement. One of these was mainly bedridden. Before treatment, one patient walked on average 326 steps a day. After six infusions of cyclophosphamide she walked 13,000 steps a day.
- We do not know whether the three patients are representative for a larger group of ME patients, but we believe that the observations can justify a clinical trial, says Fluge
The study using cyclophosphamide with six infusions, and with follow-up of 12 months, has just been approved by the Ethics Committee and the Medicines Agency. The three stressed that they have already found the patients who will participate.
- We have received letters from various parts of the world to participate in this survey. I keep getting SMS’ and emails from desperate people who ask for help, telling Fluge.
Want to reach the very sickest
40 patients, all moderately or severely ill ME, will try out the medicine. At least 25 patients will be "new", without prior rituximab treatment, while up to 15 may have gotten rituximab earlier, either without response or relapse.
- If we have a minimum 40 percent response rate among the 25 patients who have not received treatment earlier, then we will start the second part of the study, where we will try the treatment of patients who are so ill that they for years have remained at home or in nursing homes complete darkness and silence, Fluge says.
This part of the study is conceived as a collaboration between Haukeland University and local health care providers.
The Kavli Trust supports the cyclophosphamide study with a 50 percent nursing position for 12 months. The trust also finances the laboratory work related to both rituximab- and cyclophosphamide studies. The hospital does blood work of all patients included in both studies. The samples are analyzed and submitted to a bio bank.
Wants to understand disease mechanism The researchers also conducted three autopsies of people who suffered from ME.
- We are trying to understand disease mechanism. Intellectually, this work is just as interesting as watching response to disease treatment. It is this that can remove the whole management of the disease and the patient group, says Olav Mella.
Scientists estimate that 0.1-0.2 percent of the population are affected ME.
They differ between ME, defined by so-called Canadian criteria, and fatigue and burnout that can befall ten times more than those diagnosed by strict criteras. They think a lot of disagreements that have emerged is due to what one define ME to be.
- It is fascinating that some claim they are sure what ME is. We do not know what ME is. We have some hypotheses, but we do not know. There is no proof of what ME is as of today. On that basis, it is interesting that some ignore what patients has to say about their illness, says project coordinator Kari Sørland.
- We can understand that one can disagree our hypothesis for ME. However, it is incomprehensible that some rejects the idea of research and clinical trials, if these are thoughtful and performed by international guidelines, says Fluge.
From faker's disease to plaque in the brain
ME is not the first disease in history where the sick have not been believed. Multiple sclerosis (MS) was called faker's disease until the MRI apparatus was invented and found plaques in the brain. Ulcers believed came because of stress, until it was discovered a bacterium in the stomach.
Because of the high costs it is rare that such large trials that the new rituximab study is researcher driven and not initiated and run by pharmaceutical companies. The research team has received support from the Ministry of Health, the Research Council, ME Association, fundraising MEandYou besides the Kavli Trust.
Original article in Norwegian: http://kavlifondet.no/2015/03/leter-etter-svar-pa-me-gaten/
(Translated by myself with some help from Google Translate)
Last edited: