Skyline
Senior Member
- Messages
- 140
- Location
- Bangkok, Thailand
This is a thread to help me structure and track my progress and keep things controlled and get useful feedback. I'll also post summaries of what I've studied (my way of learning) that will hopefully be useful for others.
Background: Since May 2012 have had a variety of brain symptoms (headache, irritability, paranoia,altered state of consciousness), fatigue, strange nausea, vomiting, diarrhea, progressing to Neuropathy in August, blurred eyesight and unexplained fevers at times.
Test Results (received today): EBV (160:1) hs-CRP (0.34), Serum B12 (3,132 pg/ml), Homocysteine (9.68 umol/L).
Current tests on order: Yasko's Nutrigenomic's profile, 23andme, UAA/ UTM/ UEE with Yasko.
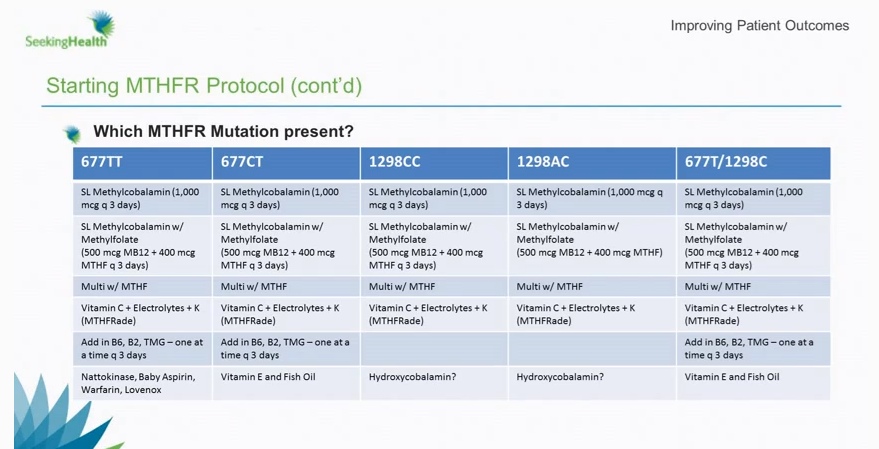
Current protocol: Fredd/ Rich Van Konyenberg methylation/ B12 protocol
Previous protocol: Jarrows Methylcobalamin 5Mg/ day for last 3 months, 1 month of Metafolin in September, vitamin D3, Vitamin K1+K2
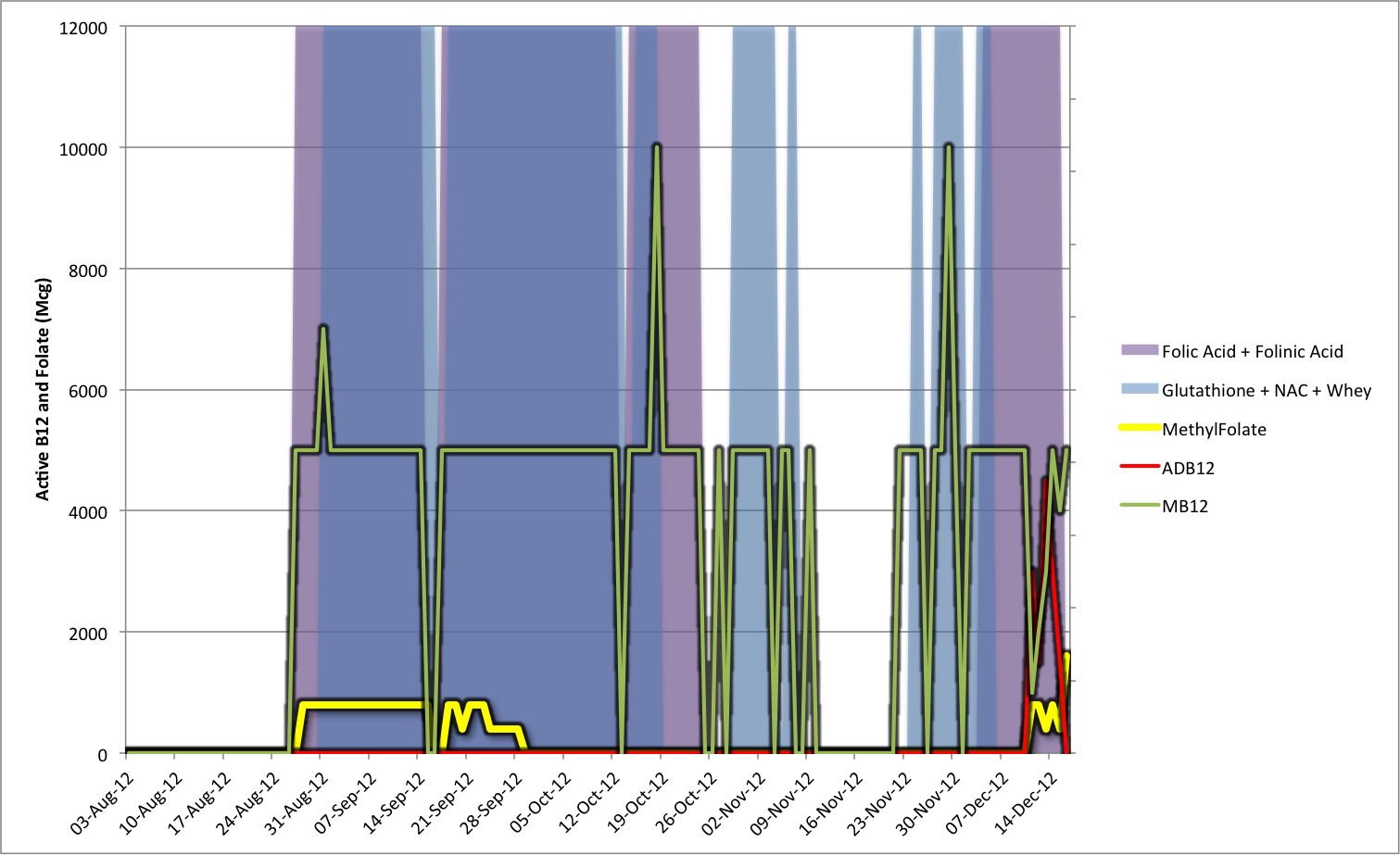
Progress: I started the methylation protocol on Tuesday 11th December with:
Solgar Metafolin: 800 Mcg
Enzyme Therapies Methylcobalamin B12: 1Mg
Country Life adenosylcobalamin B12 (Dibencozide): 3Mg
Since starting the protocol I've had a variety of more extreme neuropathies and more insomnia.
Next Steps: I'm researching the high serum B12 which I had expected to be too low - instead it is extremely high.
Background: Since May 2012 have had a variety of brain symptoms (headache, irritability, paranoia,altered state of consciousness), fatigue, strange nausea, vomiting, diarrhea, progressing to Neuropathy in August, blurred eyesight and unexplained fevers at times.
Test Results (received today): EBV (160:1) hs-CRP (0.34), Serum B12 (3,132 pg/ml), Homocysteine (9.68 umol/L).
Current tests on order: Yasko's Nutrigenomic's profile, 23andme, UAA/ UTM/ UEE with Yasko.
Current protocol: Fredd/ Rich Van Konyenberg methylation/ B12 protocol
Previous protocol: Jarrows Methylcobalamin 5Mg/ day for last 3 months, 1 month of Metafolin in September, vitamin D3, Vitamin K1+K2
Progress: I started the methylation protocol on Tuesday 11th December with:
Solgar Metafolin: 800 Mcg
Enzyme Therapies Methylcobalamin B12: 1Mg
Country Life adenosylcobalamin B12 (Dibencozide): 3Mg
Since starting the protocol I've had a variety of more extreme neuropathies and more insomnia.
Next Steps: I'm researching the high serum B12 which I had expected to be too low - instead it is extremely high.
") Could you be more specific about:
Could you be more specific about: