I have seen Rich mention this as a concern, however I would like to examine this a bit more closely. My primary issue here is with the seemingly incredible low dose of methylfolate on the Simplified Methylation Protocol. 400-800 micro grams of folate as according to RDA. But my question is since when does anyone take RDA of anything in order to get better!? When someone is sick do you recommend 60mg of VitC because that's what the RDA says?
My understanding is that RDA is one of those antiquated protocols that was based on the absolute bare minimum required of a specific nutrient to not come down with something like scurvy. And on top of that when the protocol was created back in the 60's nutrients from food were considerably more abundant due to less over-farming and less pesticide/herbicide use.
Other ND's such as Jared M.Skowron are giving child patients 10mg a day of methylfolate and having incredible results within days of administering! (source)
"A complete lack of dietary folate takes months before deficiency develops as normal individuals have about 500–20,000 µg of folate in body stores." (source - http://en.wikipedia.org/wiki/Folate)
If normal people can store folate of up to 20mg then and their reserves are constantly being topped off via diet, then yes it is reasonable to understand why RDA of folate might be so low.
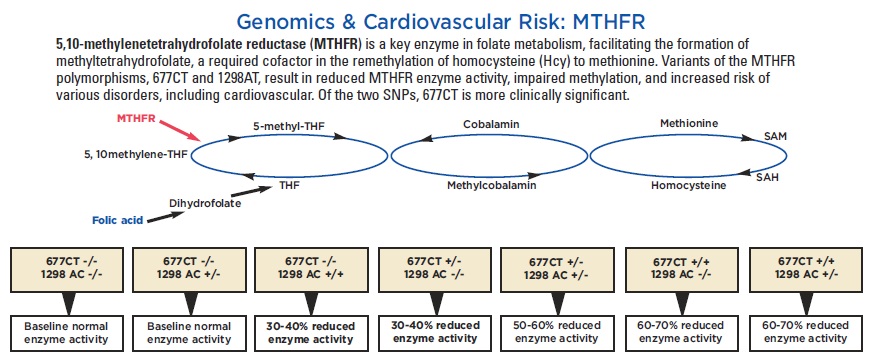
But now we must consider mutations on the MTHFr gene and prevalence. It doesn't matter how much folate your body stores or you get in your diet if you have a down regulation of 5-MTHF production.
According to Dr.Ben Lynch in regards to mutations on MTHFR C677T
1 SNP = 40% loss of function
2 SNPs = 70% loss of function
(source - http://www.seekinghealth.com/media/Improving-Patient-Outcomes-short-ver.pdf)
What's more according to statistics about 40% of people globally have an SNP on C677T. With 15% of the people having two variants, resulting in 70% loss of function. Now what is the estimated global rate of CFS/ME? Might there be a correlation?
I would venture to guess yes. Most...80%+ of people with ME/CFS probably have at least 1 if not 2 SNP's on the very gene that codes for the enzyme that creates methylfolate. This is why I believe gene testing is so important. And also why in most cases PWME need to have much higher doses of methyfolate than the RDA...
Looking a the the following results seems to prove my point.

5-MTHF levels barely moved! You could stick people on the RDA of methylfolate for years, and because of the mutaitons on the C677T gene and lack of controvertible stores, people will be chronically low and undernourished with methyfolate, and thus the whole methylation cycle will be perpetually compromised.
My contention is that people with the double mutation are required to take large doses of methyfoalte for life in order to have proper functioning methylation.
Now yes I do believe you can give someone too much methyfolate leading credence to your theory of over-driving the methylation cycle, however again, those are probably the individuals with NO SNP's on C677T, and I am willing to bet those with ME/CFS who have NO mutations are probably in the extremely low minority. Don't let the minority create a rule of thumb....
And now add to this your latest findings.
http://forums.phoenixrising.me/inde...tion-cycle-block-hypothesis-for-me-cfs.15701/
"3. The state of oxidative stress worsens as a result of the depletion of glutathione, and peroxynitrite rises, due to reaction of rising superoxide with existing nitric oxide.
7. The elevated peroxynitrite catabolizes methylfolate, preventing its rise in the plasma [NOTE: THIS STEP WAS CONTRIBUTED BY PROFESSOR MARTIN PALL, BASED ON PUBLISHED LITERATURE, FOR WHICH I AM GRATEFUL.]
8. The above process depletes the intracellular folates in general (as inferred from measurements with the methylation pathways panel)."
Ok so now the RDA of metylfoalte really isn't going to cut it, if we can expect a good portion of ingested methylfolate to be catabolized via peroxynitrate. It would be interesting to see if there was a % rate of catabolization. Is it 20% or 90%? It's probably different for everyone. Can this be measured?
In summary I really think the dosage of methylfolate needs to be examined and needs to be increased substantially. I also think genetic testing on the MTHFr gene is crucial in terms of trying to figure out proper dosage.
My understanding is that RDA is one of those antiquated protocols that was based on the absolute bare minimum required of a specific nutrient to not come down with something like scurvy. And on top of that when the protocol was created back in the 60's nutrients from food were considerably more abundant due to less over-farming and less pesticide/herbicide use.
Other ND's such as Jared M.Skowron are giving child patients 10mg a day of methylfolate and having incredible results within days of administering! (source)
"A complete lack of dietary folate takes months before deficiency develops as normal individuals have about 500–20,000 µg of folate in body stores." (source - http://en.wikipedia.org/wiki/Folate)
If normal people can store folate of up to 20mg then and their reserves are constantly being topped off via diet, then yes it is reasonable to understand why RDA of folate might be so low.
But now we must consider mutations on the MTHFr gene and prevalence. It doesn't matter how much folate your body stores or you get in your diet if you have a down regulation of 5-MTHF production.
According to Dr.Ben Lynch in regards to mutations on MTHFR C677T
1 SNP = 40% loss of function
2 SNPs = 70% loss of function
(source - http://www.seekinghealth.com/media/Improving-Patient-Outcomes-short-ver.pdf)
What's more according to statistics about 40% of people globally have an SNP on C677T. With 15% of the people having two variants, resulting in 70% loss of function. Now what is the estimated global rate of CFS/ME? Might there be a correlation?
I would venture to guess yes. Most...80%+ of people with ME/CFS probably have at least 1 if not 2 SNP's on the very gene that codes for the enzyme that creates methylfolate. This is why I believe gene testing is so important. And also why in most cases PWME need to have much higher doses of methyfolate than the RDA...
Looking a the the following results seems to prove my point.
5-MTHF levels barely moved! You could stick people on the RDA of methylfolate for years, and because of the mutaitons on the C677T gene and lack of controvertible stores, people will be chronically low and undernourished with methyfolate, and thus the whole methylation cycle will be perpetually compromised.
My contention is that people with the double mutation are required to take large doses of methyfoalte for life in order to have proper functioning methylation.
Now yes I do believe you can give someone too much methyfolate leading credence to your theory of over-driving the methylation cycle, however again, those are probably the individuals with NO SNP's on C677T, and I am willing to bet those with ME/CFS who have NO mutations are probably in the extremely low minority. Don't let the minority create a rule of thumb....
And now add to this your latest findings.
http://forums.phoenixrising.me/inde...tion-cycle-block-hypothesis-for-me-cfs.15701/
"3. The state of oxidative stress worsens as a result of the depletion of glutathione, and peroxynitrite rises, due to reaction of rising superoxide with existing nitric oxide.
7. The elevated peroxynitrite catabolizes methylfolate, preventing its rise in the plasma [NOTE: THIS STEP WAS CONTRIBUTED BY PROFESSOR MARTIN PALL, BASED ON PUBLISHED LITERATURE, FOR WHICH I AM GRATEFUL.]
8. The above process depletes the intracellular folates in general (as inferred from measurements with the methylation pathways panel)."
Ok so now the RDA of metylfoalte really isn't going to cut it, if we can expect a good portion of ingested methylfolate to be catabolized via peroxynitrate. It would be interesting to see if there was a % rate of catabolization. Is it 20% or 90%? It's probably different for everyone. Can this be measured?
In summary I really think the dosage of methylfolate needs to be examined and needs to be increased substantially. I also think genetic testing on the MTHFr gene is crucial in terms of trying to figure out proper dosage.