Dr. Yes
Shame on You
- Messages
- 868
I think you're right, Lily.. that last sentence of mine was mostly wishful thinking, practically speaking...

Welcome to Phoenix Rising!
Created in 2008, Phoenix Rising is the largest and oldest forum dedicated to furthering the understanding of, and finding treatments for, complex chronic illnesses such as chronic fatigue syndrome (ME/CFS), fibromyalgia, long COVID, postural orthostatic tachycardia syndrome (POTS), mast cell activation syndrome (MCAS), and allied diseases.
To become a member, simply click the Register button at the top right.
I like this, with the exception that not all neurological illnesses are characterized by PEM. So one could say "graded exercise is as useful in treating ME as it is in any other disease in which graded exercise, or any other minimal exertion, increases morbidity." CAA should just say a more concise version of this: "GET is contraindicated in treating ME/CFIDS." Period.
Some patients become fearful that any exertion will trigger symptoms (kinesophobia), and thus become couch- or bedbound. This, however, only leads to stiffness, soreness, and severe deconditioning. Such individuals are encouraged to initiate a progressive program of stretches and range-of-motion activities and then add low-level physical activities like short walks or floating in a pool.
Cort wrote:
I'm not particularly excited about this
I'm glad to see that all of you took a look at the parts of the CME that I posted.
Dr. Yes, when I said that I thought the new CME was a whole lot better than the old one, I had not read further down it yet where they started talking about CBT, GET and making disparaging comments. As I went along, I expressed my dismay at what I was finding. I suppose I should have gone back and erased my initial reaction because I do not stand by that statement now that I've finished reading the CAA's Continuing Medical Educational materials for our doctors.
I've had it with the CAA! I agree that you all are right, and I'm appalled at what they have done to us again and again.
I hold the CAA directly responsible for miseducating our doctors and the public. It's their fault that we're being treated like lazy malingering hypochondriacs.
from from the CAA info (someone else quoted this, i have not read through all the info yet):
>
It might be easy to not get too excited about it if you feel it is not about you. However this sort of nonsensical statement (re exercise phobia) needs challenging. This is not just because it is unsubstantiated CBT school rubbish, not just because the more severe a patient the more vulnerable they are to the abuse and ignorance of others (and at a time when they most need help), but also because this sort of thinking affects all of us.
[Edit: and the above statment gives the impression that peope become severe because of phobia. For people who are severe it could be very bad if everyone around them, that they are utterly dependent on, started to think this way, it could be a great excuse to neglect them and not meet basic needs.]
Once it is hinted at that some patients are phobically avoiding activity, the air of suspicion cloaks us all, whether we like it or not. Once this idea is out there at all as a serious idea, every time you see a new doctor, every time someone in authority makes a decision about your disability, housing, home help, testing or about any assistance you might apply for, they might have this niggling doubt at the back of their mind that maybe you could just do a bit more, and maybe you are just phobically avoiding activity, so maybe they are not helping you by giving you things.
There is no evidence that phobic avoidance of activity is a general problem in ME/CFS. Yes maybe you could find one in a million that fit this model to some extent (though if they have ME/CFS they still have a problem with exercise, whether they are phobic or not), but is it worth hanging the rest of us for this? This comment about phobia will only encourage and indulge the most ignorant doctors to feel that they were right all along, and it might put the idea into the heads of good doctors.
Well then that is a depression problem and not an ME/CFS one, and once the depression is dealt with they still have ME/CFS so need to be careful about not overdoing it.
<
No they will very likely get worse from trying to exercise, unless they are improving naturally. I have known people to try very gentle exercises when bedbound and it was an absolute fiasco. Like the rest of us, if the severe patient improves they will start to do more. They are not more severe because they are phobic but because of the nature of the illness (and I am not saying there is not the odd patient out there who couldn't manage better, but again why hang the vast majority for this?).
But there is no evidence that this is appropriate or helpful.
Well not as bad as ME/CFS. And the word deconditioning is thrown about far too much. Muscle wastage is almost unheard of in ME/CFS and blood clots are rare. One difference between ME/CFS patients and patients with paralysis is that ME/CFS patients are normally moving around to some extent so they avoid some of the problems typically associated with deconditioning.
There are also other ways around exercise for dealing with some potential problems in the very severe, for example using splints where necessary. But some physio's can even resist this if they think the patient needs encouragement to do exercises (I know of more than one person this has happened to. I remember reading of one case where splints were removed, and the patient ended up with a problem than they need not have had, all because the people treating the patient thought they should be excercising).
Maybe, when more is known about ME/CFS physiology physiotherapy can be more safely administered but at the moment they are basically clueless about what they are doing treatment-wise, and it is all a guessing game, and as far as I am concerned our guess is better than theirs.
Orla
I'm not particularly excited about this but then again in a community of 1,000,000 people some people are going to do this. How could that not happen? Some people are depressed - there's going to be a range of reactions to CFS. I would imagine that many people who are bedbound who follow the appropriate 'exercise' therapy are probably still bedbound but are stronger for it and are less deconditioned, etc. There's no talk of a cure because there's no expectation - just improving their health a bit. They talk about starting 'range-of-motion activities' and stretching - things we wouldn't ordinarily think to do. Deconditioning is a terrible burden to place on a body. .
They also need to state that patients on the other hand are simply so ill that they become bedbound.
This is Dr. Bateman, Dr. Lapp and the CAA talking - those doctors have seen 1,000's of patients, Teej, I think they do get it about CFS. I know how its troubling but they're talking about one type of patient that they do come across not the general set of patients. Glad you like the program more than the last one")
from from the CAA info (someone else quoted this, i have not read through all the info yet):
>
It might be easy to not get too excited about it if you feel it is not about you. However this sort of nonsensical statement (re exercise phobia) needs challenging. This is not just because it is unsubstantiated CBT school rubbish, not just because the more severe a patient the more vulnerable they are to the abuse and ignorance of others (and at a time when they most need help), but also because this sort of thinking affects all of us.
[Edit: and the above statment gives the impression that peope become severe because of phobia. For people who are severe it could be very bad if everyone around them, that they are utterly dependent on, started to think this way, it could be a great excuse to neglect them and not meet basic needs.]
Once it is hinted at that some patients are phobically avoiding activity, the air of suspicion cloaks us all, whether we like it or not. Once this idea is out there at all as a serious idea, every time you see a new doctor, every time someone in authority makes a decision about your disability, housing, home help, testing or about any assistance you might apply for, they might have this niggling doubt at the back of their mind that maybe you could just do a bit more, and maybe you are just phobically avoiding activity, so maybe they are not helping you by giving you things.
There is no evidence that phobic avoidance of activity is a general problem in ME/CFS. Yes maybe you could find one in a million that fit this model to some extent (though if they have ME/CFS they still have a problem with exercise, whether they are phobic or not), but is it worth hanging the rest of us for this? This comment about phobia will only encourage and indulge the most ignorant doctors to feel that they were right all along, and it might put the idea into the heads of good doctors.
Well then that is a depression problem and not an ME/CFS one, and once the depression is dealt with they still have ME/CFS so need to be careful about not overdoing it.
<
No they will very likely get worse from trying to exercise, unless they are improving naturally. I have known people to try very gentle exercises when bedbound and it was an absolute fiasco. Like the rest of us, if the severe patient improves they will start to do more. They are not more severe because they are phobic but because of the nature of the illness (and I am not saying there is not the odd patient out there who couldn't manage better, but again why hang the vast majority for this?).
But there is no evidence that this is appropriate or helpful.
Well not as bad as ME/CFS. And the word deconditioning is thrown about far too much. Muscle wastage is almost unheard of in ME/CFS and blood clots are rare. One difference between ME/CFS patients and patients with paralysis is that ME/CFS patients are normally moving around to some extent so they avoid some of the problems typically associated with deconditioning.
There are also other ways around exercise for dealing with some potential problems in the very severe, for example using splints where necessary. But some physio's can even resist this if they think the patient needs encouragement to do exercises (I know of more than one person this has happened to. I remember reading of one case where splints were removed, and the patient ended up with a problem than they need not have had, all because the people treating the patient thought they should be excercising).
Maybe, when more is known about ME/CFS physiology physiotherapy can be more safely administered but at the moment they are basically clueless about what they are doing treatment-wise, and it is all a guessing game, and as far as I am concerned our guess is better than theirs.
Orla
It is not a whole lot better; on the contrary, it is more of the same.. so much so that I don't even know where to begin and don't have the energy to even begin to address all the problems right now. I don't know why I or anyone else should have to, frankly. But basically...
I find this new CME disturbing in some of the same old ways... perhaps because much of it seems to be recycled material from their website or other literature. There's a bit more that is good, but much of that ends up contradicted or countermanded by parts that are bad (sound familiar?). In the section on pacing that precedes the sections quoted above, everything is fine; then they get to strength and conditioning, where the usual problem of lack of clarity begins - is this for all patients? THAT much activity.. for whom?? Note that they are essentially promoting low-level graded exercise there. Then they go on to promote GET - again!! What so many of us have been pushing for was to get rid of GET (and CBT) from CAA literature! Yet again, they claim it has been found to help with fatigue, exhaustion, whatever.. based on those same highly questionable studies; more on that later. This is the same kind of stuff from the SPARK material, stuck in the middle of a jelly donut.
Even more ridiculous: the bit quoted in other posts about 'activity phobia' such that 'some' lie around on couches.. Orla just attacked that point, and rightly so; it is something to SCREAM at the CAA about! There, and in the part about some patients inappropriately avoiding activity for fear of repercussions, they are continuing to spread the myth of hypochondriacal or 'symptom-exaggerating' or neurotic patients to our doctors; they are STILL spreading the damaging B.S. that is screwing a lot of people right now, including me.
Read through it again, if you hadn't noticed what I pointed out so far. It's the same old stuff - not as much of it, and with a few bonbons thrown our way, but the core problems remain. There is no way that an ME/CFS advocacy group should have found this suitable to disseminate to the medical community. I don't want to hear the cliche about throwing out the baby with the bathwater again - I have a better one: this is (should be) OUR literature and we can have our cake and eat it too. We don't need to settle for something inadequate or less. Significant sections of this new CME are just as confusing and potentially damaging as certain other attempts at decent information by the CAA; other bits of it - as pointed out by others - are simply shameful, and I hope fervently for my own sake that neither my current nor my future doctors ever see this. And if any of us have to be afraid that our doctors will see this, then what the heck good is it?
The CAA really needs our help. And they need to trust US, for whom they advocate, above all others.
I'm going to stop reading/commenting on this thread. The CAA needs to be held responsible for a lot of things. But you CANNOT say that they are directly reponsible for this. The education provided by Drs. Bateman and Lapp is the only thing I've ever seen that even comes close to providing worthwhile and valid information for physicians regarding ME/CFS. Some of the other information the CAA has posted, yes, they should have known better.
Once again, you are going overboard. The issues with this CME should be directed to Drs. Bateman and Lapp, not the CAA.
What about the CCC article? I think it was 100% accurate. CAA should just put up that article.
<Maybe, when more is known about ME/CFS physiology physiotherapy can be more safely administered but at the moment they are basically clueless about what they are doing treatment-wise, and it is all a guessing game, and as far as I am concerned our guess is better than theirs.>
Orla
Yes, this would seem to be common sense, but common sense isn't very common when it comes to this subject.
All this talk of "coping" and how exercise/activity might treat symptoms has been inherited from the school of "thought" that assumes WE are what is wrong with US. That WE don't know how to behave in our own best interests, that WE somehow are totally responsible for our condition and other people's response to it/us. It is just more of the campaign to direct attention away from the biomedical facts of our lives and redirect attention, and research money, toward more wheel-spinning, directionless buzz.
CONCLUSION: The data suggest that CFS patients without a comorbid psychiatric disorder do not have an exercise phobia.
IS THE CHRONIC FATIGUE SYNDROME AN EXERCISE PHOBIA? A CASE CONTROL STUDY
Gallagher AM, Coldrick AR, Hedge B, Weir WR, White PD.
J Psychosom Res. 2005 Apr;58(4):367-73
Cort wrote: This is Dr. Bateman, Dr. Lapp and the CAA talking.
How did Reeves survive his involvement with this crime of years’ duration? After all, the slush fund was public knowledge by 1996, and Congress and its investigative arm, then the General Accounting Office or GAO, and the Department of Health and Human Services, were exploring the possibility of launching investigations. Here's how he survived: In 1998 Reeves stepped forward, claiming protection under the Federal Whistleblower Act. This allowed him to reveal the theft of money but suffer no consequences. The Act offers its beneficiaries perpetual freedom from being fired in return for exposing waste or fraud. Reeves bought himself another twelve years in the “cfs” field this way. Those of you who think that was a good thing can send your “thank you” notes to Kim Kenney of the CAA, who supported Reeves in this false act of public contrition and presented him to patients and the media as a hero of conscience. (“The Association was instrumental in Reeves’ effort to call attention to the misspending of CFIDS funds…” [CFIDS Chronicle, May/June 1999], and “Reeves sought assistance from The CFIDS Association in taking his documentation to the right people in government. Kim Kenney, Tom Sheridan and Doralee Halperin helped him prepare for the meetings, accompanied him to them and have continuously followed up since.” [Ibid., 1998, September/October])
Here's the 2000 GAO report where you can read the GAO's conclusions about the agency's accounting practices under, "Accounting Issues at CDC."
HJ writes: The agency as a whole [the CDC] also grew more sophisticated about controlling the flow of information about the disease and its scientists' activities. It did so by using a lot of in-house marketing and public relations expertise, building a website that brims with disinformation and engaging the CAA to educate MDs and further burnish the “cfs” brand in the U.S. and elsewhere. Reeves held sway over the bitterly contested “empirical definition” and the way-out-there genomic study, which in turn led to the infamous press conference of 2006, in which Reeves and his collaborator Suzanne Vernon proposed that the disease was under diagnosed by 80 percent, that treatment was available, and that “cfs” was caused by a genetic predisposition to being unable to handle stress combined with a history of child abuse.
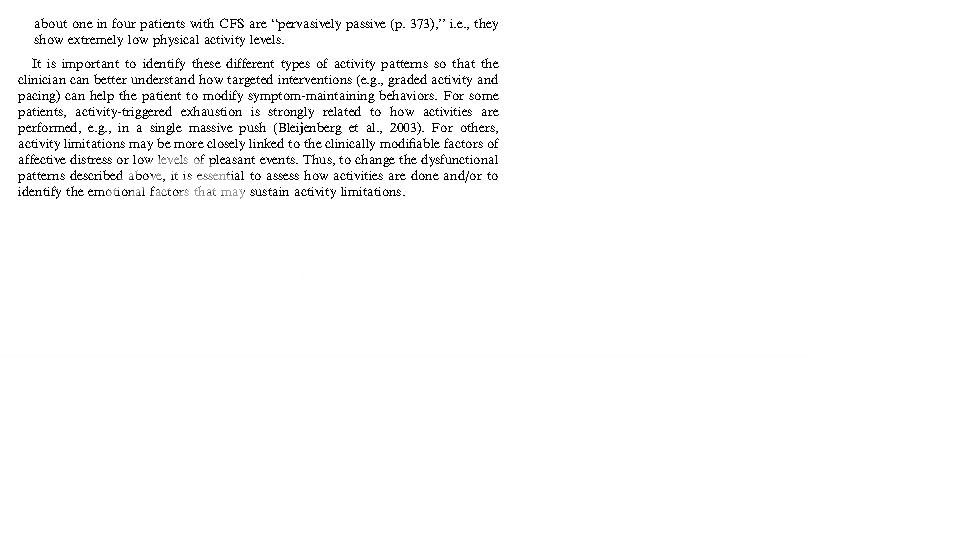
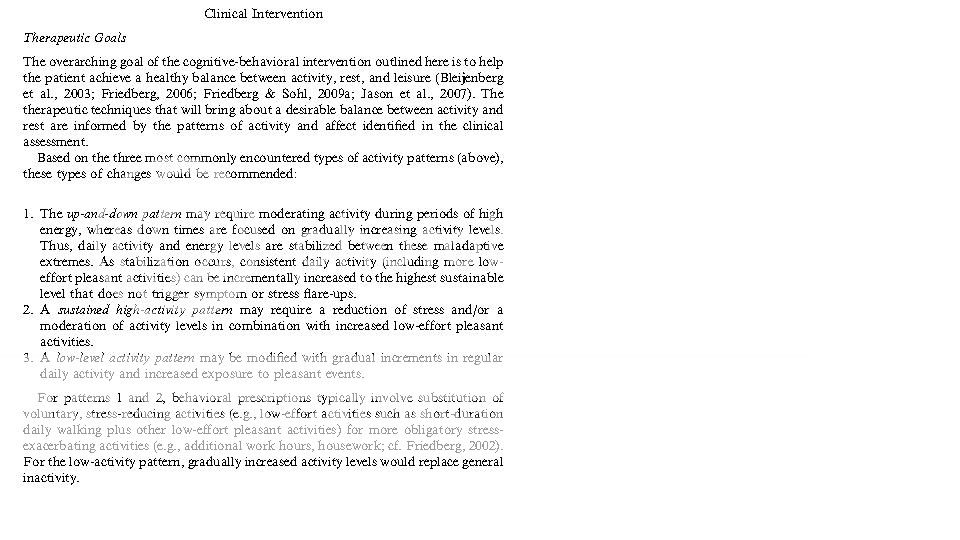
I'm not up-to-date on this thread but I heard 1+ person(s) was doubting this so I thought one way to resolve this was to post the images from this recent (2010) paper:Fred Friedberg is now recommending graded activity for the quarter of patients who are least active. For other groups, he is more nuanced. (Not sure how relevant that is to the CAA but my overall point is that I don't think the professionals necessarily get the issue).

Hi Oerganix,
Just to be clear, when I said
To which you answered:
In case I was misunderstood in what I meant, I didn't mean physio to administer GET because of phobic avoidance or any of that nonsense. I meant that it is possible that they might have some minor role to play in a minority of cases, but not to administer GET. Sometimes some physio (massage I think) can be useful for pain in some other conditions, though in ME/CFS they are probably more likely to cause it than help it, certainly at the moment.
Of course ME/CFS is different from things like MS that can benefit from physio, partly because of the nature of the disability itself, and partly because of the degree of exercise intolerance in ME/CFS, which most non-ME/CFS people find hard to get their head around. But I feel I cannot completely rule out a future role, in a minority of cases, but feel at the moment it is generally a dangerous route to go down. I also would not be in favour of spending money on researching physio for ME/CFS at the moment, and would prefer the money to go towards trying to understand the underlying pathophysiology. Maybe you understood this from what I said, but just in case people hadn't seen my other stuff on GET/CBT I thought I should clarify.
To be honest I think it is likely that if there is useful biomedical treatment that the whole debate will move over to biomedical treatment, and maybe all this stuff about exercise and so on will become irrelevant? Though that is unlikely to happen for a while, unfortunately.
Edit: Meant to say good post Mithriel. And I didn't think to say yesterday that a phobia has a meaning in psychology. In the context of exercise phobia, it wouldn't just indicate a worry about exercise/activity, but an irrational fear of exercise/activity and total panic if made to do things. I have never come across a patient that comes close to this description.
And a study involving Peter White did not find evidence of exercise phobia. Gracenote posted about this on the psychiatric theory thread.
Orla