Promising, but not there yet
I really like what the authors are trying to do here - look at how gene expression in CFS patients differes from controls after moderate exercise - but I think the results are compromised by the fact that the exercise was not always moderate for CFS patients. Here's what they tried to do:
We elected to use a sustained moderate exercise rather than a maximal exercise test (which typically last only 5-9 min in CFS patients) because of closer similarity to the natural exercise experiences reported to exacerbate CFS symptoms in patients daily lives
...
We attempted to adjust for fitness level mismatches by exercising all patients and controls at the same relative exercise intensity, to 70% of age predicted, maximal heart rate.
The problem with this approach is that for the most severely affected patients (bedbound/housebound) 70% of max heart rate for 25 mins is way, way more than moderate exercise and is vastly more than "natural exercise experiences reported to exacerbate CFS symptoms in patients daily lives". I would be in the second most severe category, 'could live alone with occasional help' and know from trying in the past that I could only manage 70% of max heart rate for a few minutes - my problems are caused by activity way below this.
The mean score for self-rated exertion for the control group was 3.1, which is just right as a score of 3 equates to moderate exertion. For the CFS group the mean was 5.0 ('hard' exertion) but would have been substantially higher than this for some patients.
[from other data given, the exertion for the 21 most exhausted patients can be calculated as 6.5, equivalent to 'very hard' exertion]
This matters, because the genes chosen for study have increased expression for strenous exercise in
healthy controls:
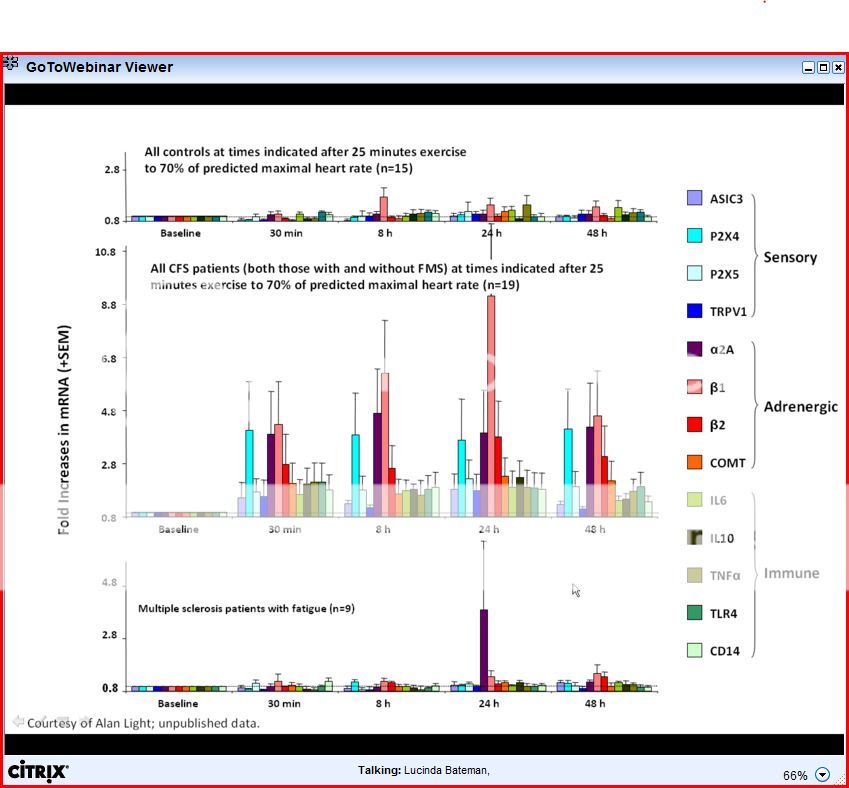
Initial experiments with normal subjects indicated that mRNA for [genes in this 2011 study] was upregulated at 8 and 24 hours after strenuous exercise. (from 2009 pilot study)
Worryingly, figure 3 shows that the biggest increases by far for gene expression are in the two most severely affected groups whose exercise level is likely to be far above moderate. It could be argued this is exactly as expected for individuals exercising very hard, not evidence for a specific disease process.
Now, as Dolphin noted, the authors do address this point by an analysis that only looked at patients and controls with similar exertion levels:
This comparison examined 15 controls with the highest RPE (mean 3.89) matched with 27 patients with overlapping RPEs (mean 3.87). Even though this reduced our sample size and statistical power substantially, 6 of the 7 genes AUCs were still significantly greater in CFS patients than controls [P2X4 (p<.05), TRPV1 (P<.02), -2A (P<.03), -2 (P<.03), COMT (P<.04), and IL10 (P< .01)]. The only gene not reliably different was P2X5 (P=.12)
This is an important finding. However, the statistical significance is much less impressive than for the full study (no doubt due to losing the patients with the biggest differences, as well as the inevitably smaller sample size) and the sample size is small. We don't know if the alpha-2a subgroup exists in this smaller sample.
What this leaves us with is effectively a pilot-study type result (15 controls/27 patients vs 49/48 in the full study), rather than a confirmatory result. It's still very interesting, but it's not nearly as convincing.
Well, that's my take. I'm happy for anyone to point out flaws in my logic. Otherwise, to be convinced I'd like to see rersults for a much larger study and ensure that exertion/exercise levels are appropriate for the level of severity experienced by each CFS patient.